Contents
Anthropometry Domain
IntroductionSubjective methods- Introduction to Subjective Methods
- Birth weight
- Body shape
- Weight and height
- Waist and hip circumference
- Introduction to Objective Methods
- Simple measures - stature
- Simple measures - weight
- Simple measures - circumference
- Simple measures - arm anthropometry
- Simple measures - skinfolds
- Simple measures - abdominal sagittal diameter
- Simple measures - head circumference
- Bioelectric impedance analysis
- Multi-component models
- Hydrostatic underwater weighing
- Air displacement plethysmography
- Hydrometry
- Whole body DEXA scan
- Near infrared interactance
- Whole body counting of total body potassium
- 3d photonic scan
- Magnetic resonance imaging (MRI) / Magnetic resonance spectroscopy (MRS)
- Total body electrical conductivity (TOBEC)
- Computed tomography (CT)
- Ultrasonography
- Introduction anthropometric indices
- Body mass index
- Fat and fat free mass indices
- Ponderal index
- Percentiles and Z-scores
- Anthropometry Video Resources
- Height procedure
- Protocol for measuring waist circumference
- Measuring hip circumference
- Weight and body composition procedure
Multi-component models
Multi-component models of body composition are a class of inference models that use more than one source of measurement data to achieve a more valid estimate of body composition.
The human body can be described in terms of its different components (or “compartments”), each of which contains different types of atomic, molecular, cellular or tissue material. These components can be assessed and combined to describe the composition of the human body; as described in Table 1, models typically use between 2 and 4 components, but 5- and 6-component models also exist The components which comprise different multi-component models are summarised in Figure 1.
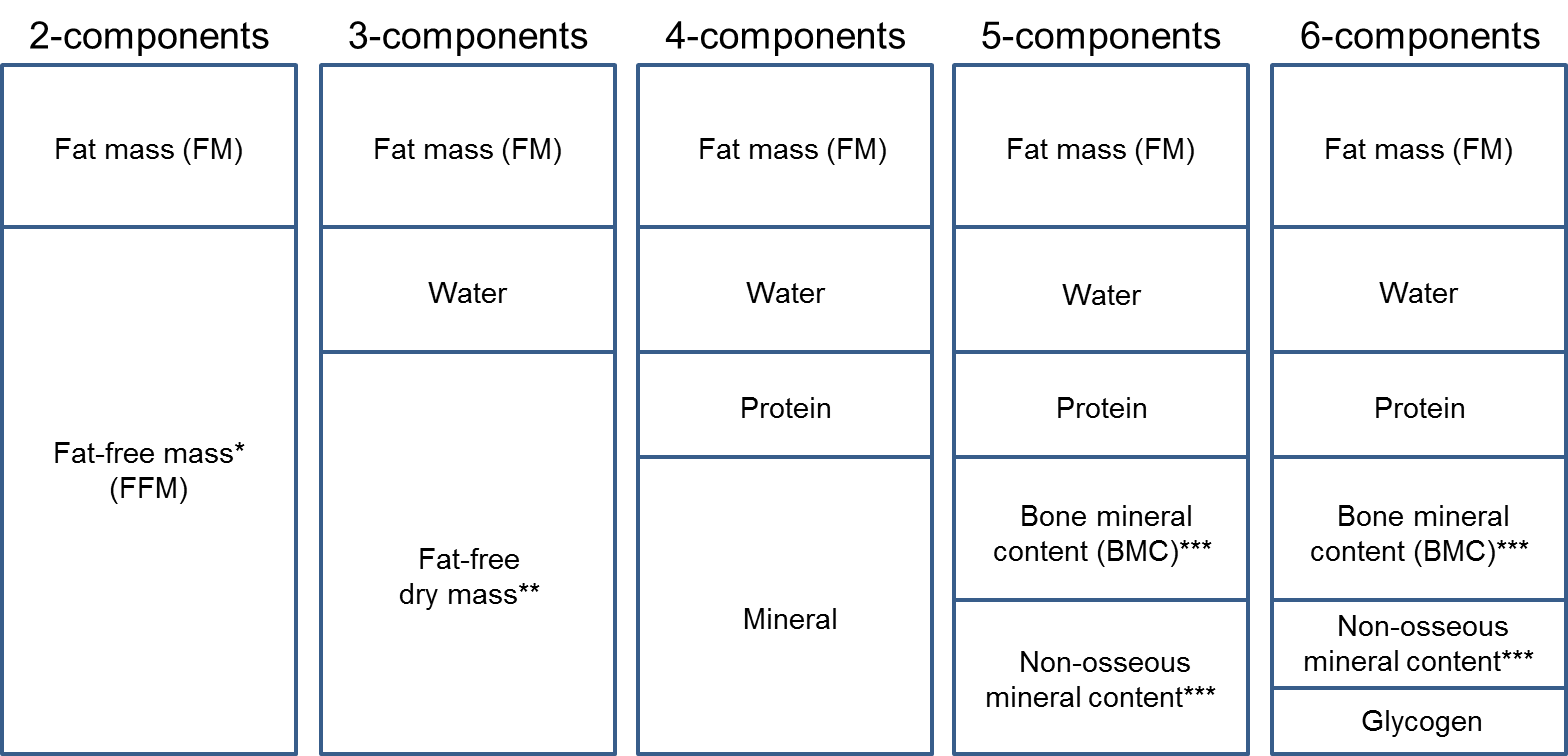
Figure 1 Components measured to generate different multi-component models.
Source: MRC Epidemiology Unit.
Important: Figure is not to scale and represents the assumptions of the models, not the exact relationships between different components in-vivo.
*Includes water, protein, glycogen, bone mineral content, and non- osseous mineral content.
**Includes protein, glycogen, bone mineral content, and non-osseous mineral content.
***There is a difference between mineral content and mineral mass. Measures of mineral content are typically converted to mineral mass to reflect the ashing process.
2-component models
Assessment of body composition requires quantification of at least two components; we refer to this as a 2-component (2C) model, the most common of which divides total body mass into fat-free mass (FFM) and fat mass (FM).This model assumes that fat-free mass and fat mass have densities of 1.1 kg/L and 0.9 kg/L respectively and this approach typically uses the following equations to estimate % body fat:
- Siri (1956): Fat % = [4.950 /Density - 4.500]*100
- Brozek et al. (1963): Fat % = [4.570 /Density - 4.142]*100
Measurements that allow inferences to be made on these components include:
- Bioelectrical impedance analysis
- Whole body counting of total body potassium
- Densitometry methods:
- Hydrostatic underwater weighing
- Air displacement plethysmography
- Hydrometry (isotope dilution)
However, the 2C model is subject to error due to inter-individual variation in the composition of the fat-free mass compartment. Fat-free mass consists of minerals, proteins and water. The 2C model assumes constant values for water content (hydration fraction), bone mineral content (BMC), and density of fat-free mass, but these do vary between ethnicities, age groups, pubertal status, pregnancy, weight loss status, and in patients with deranged hydration (e.g. chronic renal failure, cirrhosis). The 2C model is therefore not ideal for assessing fat-free mass under these conditions and circumstances.
3- and 4-component models
Models that assess 3 or 4 components expand upon 2-component models by measuring fat-free mass constituents with greater certainty. The 3-component (3C) model divides body mass into fat, water, and fat-free dry mass (proteins and minerals). This model avoids the assumption that water content of fat-free mass is constant between individuals, however the ratio between the proteins and minerals of fat-free dry mass is assumed to be constant. This model requires the following data:
- Body mass
- Body volume from densitometry (e.g. under water weighing or air displacement plethysmography)
- Total body water (stable isotope dilution analysis or bioelectrical impedance analysis)
The 4-component (4C) model further divides fat-free dry mass into protein and bone mineral content (BMC). This model requires the same information applied in the 3C approach, with the addition of the measurement of bone mineral content by dual-energy X-ray absorptiometry) Estimating bone mineral content and protein mass avoids the assumption that the protein-to-mineral ratio in fat-free mass is constant; the 4C model still assumes that the ratio between bone mineral and non-osseous mineral content is constant. However, this model is robust to major differences in this ratio.
Table 1 Summary of differences between 2-, 3-, and 4-component models.
| Model | Components | Measurements needed | Assumptions relating to composition |
| 2-component model |
1. Fat mass
2. Fat-free mass |
Densitometry*
or Hydrometry or Bioelectrical impedance analysis or Whole body counting of total body potassium |
Constant density of fat-free mass
Constant water content of fat-free mass Constant bone mineral to muscle ratio in fat-free mass |
| 3-component model |
1. Fat mass
2. Water 3. Fat-free dry mass |
Densitometry*
and Hydrometry |
Constant protein-to-mineral ratio of fat-free dry mass |
| 4-component model |
1. Fat mass
2. Water 3. Protein 4. Bone mineral content |
Densitometry*
and Hydrometry and Dual-energy X-ray absorptiometry (DEXA) |
Constant bone mineral content to non-osseous mineral content ratio |
*Densitometry methods include: hydrostatic underwater weighing and air displacement plethysmography.
5- and 6-component models
Other models have been developed, which assess 5-6 components. The five component model (5C) divides total body mass into water, fat mass, protein mass, bone mineral mass and non-osseous mineral mass (notably soft tissue minerals). While, the six component model developed by Wang et al. (2015), includes estimates for residual mass components soft tissue mineral and glycogen.
However, these models are used less frequently than the 4C model, which is considered the reference method for the in-vivo assessment of overall body composition (but not for fat distribution). It is robust to inter-individual variability in the composition of FFM as more measurements are performed on this compartment, thus the inference requires fewer assumptions.
Several measurements are required to construct 3C and 4C models, as shown in Table 1. Information about these methods is available on separate pages.
Body weight and body volume are measured using densitometry (e.g. hydrostatic underwater weighing or air displacement plethysmography) and total body water is measured using hydrometry (isotope dilution) or bioelectric impedance analysis if following the 3C model.
For the 4C model, the same data applied in the 3C approach are used, with the addition of the measurement of bone mineral content (BMC) using dual-energy X-ray absorptiometry (DEXA).
- 3C and 4C models are typically used as criterion measures to assess the validity of 2C models and field methods (e.g. weight, height, skinfolds, circumference measurements and their combination in prediction models).
- As different body composition measurement techniques are required to calculate multi-component models, their use is restricted in large-scale population studies, in clinical practice and in field settings.
Taking into account the various assumptions underlying the densities and constant ratios (protein-to-mineral ratio in the 3C model; and the bone mineral content to non-osseous mineral ratio in the 4C model), fat mass can be estimated from the combined measurements of:
- Body mass
- Body volume from densitometry (hydrostatic underwater weighing or air displacement plethysmography)
- Total body water (isotope dilution or bioelectrical impedance)
The above measures are combined using the formulae in Table 2. There are different equations available for the same input variables but their output results for fat mass are very similar as they are all based on similar assumptions. They share assumed constant densities for fat 0.9007 g/cm3, water (0.99371 g/cm3 and for bone mineral (2.982 g/cm3), but two different approaches are taken in developing the equations:
- The residual of body mass after subtraction of fat, water and bone mineral is assumed to be composed of protein and non-osseous minerals of known densities.
- The body mass residual described in approach 1 is assumed to be a single combined residual mass (e.g. protein, non-osseous minerals and other constituents like glycogen) of known density.
Table 2 shows a selection of multi-component models to estimate overall body fat. In these models, four quantities are measured: body volume, total body water, bone mineral and body mass.
Table 2 Selection of multi-component models to estimate overall body fat mass.
| Models | Equations |
|---|---|
| 3-component model |
|
| 1 Siri (1961) | FM = 2.057*BV-0.786*TBW-1.286*BM |
| 2 Lohman (1986) | FM = 6.386*BV+3.961*M-6.09*BM |
| 3 Silva (2004) | FM = 2.122*BV-0.779*TBW-1.356*BM |
| 4- to 6-component models |
|
| 4 Selinger (1977) | FM = 2.747*BV-0.714*TBW+1.129*Mo-2.037*BM |
| 5 Lohman (1992) | FM = 2.747*BV-0.714*TBW+1.146*Mo-2.053*BM |
| 6 Heymsfield et al. (1990) | FM = 2.748*BV-0.6744*TBW+1.4746*TBBA-2.051*BM |
|
7 Baumgartner et al. (1991)
|
FM = 2.747*BV-0.7175*TBW+1.148*Mo-2.058BM |
| 8 Fuller et al. (1992) | FM = 2.747*BV-0.710*TBW+1.460*TBBA-2.05*BM |
| 9 Withers et al. (1992) | FM = 2.513*BV-0.739*TBW+0.947*Mo-1.790*BM |
| 10 Friedl et al. (1992) | FM = 2.559*BV-0.734*TBW+0.983*Mo-1.841*BM |
| 11 Siconolfi et al. (1995) | FM = 2.7474*BV-0.7145*TBW+1.1457*Mo-2.0503*BM |
| 12 Heymsfield et al. (1996) | FM = 2.513*BV-0.739*TBW+0.947*Mo-1.79*BM |
| 13 Forslund et al. (1996) | FM = 2.559*BV-0.734*TBW+0.983*Mo-1.841*BM |
| 14 Wang et al. (2002)a | FM = 2.748*BV -0.699*TBW+1.129*Mo-2.051*BM |
| 15 Wang et al. (2014)b | FM = 2.720*BV -0.715*TBW+1.108*Mo-2.020*BM |
Adapted from Wang (2005) and Heymsfield et al. (2015).
BM = Body mass (kg); BV = body volume (L); FM = fat mass (kg); M= total mineral mass (kg); Mo = bone mineral mass (kg); TBBA = total body bone ash (kg); TBW = total body water (L).
Total mineral mass (M) includes bone mineral mass (Mo) and non-osseous mineral mass.
Bone mineral mass (Mo) includes total body bone ash (TBBA) and non-osseous mineral mass.
a5-component equation.
b6-component equation.
Some equations in Table 2 require that the bone mineral content from DEXA is converted to bone mineral mass (Mo) or total body mineral mass (Mo + non-osseous) in Table 2.
Body mineral content or total body bone ash (TBBA) is typically converted to bone mineral mass (Mo) by multiplying TBBA*1.0436. This is to reflect the ashing process. Most DEXA systems have adjusted for this process (see Heymsfield 2015).
Different conversion factors also exist for the derivation of total body water mass from labelled water dilution volumes. Each equation takes a different strategy to derive soft non-osseous mineral mass. Non-osseous minerals, glycogen and other residual mass components are taken into account. Refer to each equation for the various strategies/assumptions and conversation factors (see reference list).
An overview of multi-component models is outlined in Table 3.
Strengths
- Multi-component models address variability in fat-free mass by providing information on hydration, density and mineralization of fat-free mass, this is especially important in those populations who deviate from the fixed constants assumed in 2C models (e.g., ethnicity, pregnant women, children or older individuals, disease groups and obesity).
Limitations
- Each component of the models incurs a separate cost for collection and data processing; the more components measured, the higher the final cost.
- Lack of accessibility of the different equipment used to assess the various components.
- The techniques require a multitude of expertise in collection and analysis and therefore may be suitable for a research setting but not within the practicalities of a clinical setting.
- Significant differences found in bone mineral content estimates between DEXA systems resulting in differences within the prediction models. For instance when comparing GE Lunar iDXA to Hologic Discovery A. The two estimates of bone mineral mass are highly correlated (R2, 0.98;P < 0.001), but the iDXA values are significantly larger by 13.3 ± 3.6% than the values by the Discovery A (2.76 ± 0.56 kg vs. 2.44 ± 0.47 kg; P < 0.01). The between-manufacturer mean difference in bone mineral estimates has been found to lead to a 0.6% fat unit difference in percentage body fat when applied in the 4C model.
- A whole body composition method only; it is not able to provide information on regional distribution of tissue or depots.
- The assessment of bone mineral content by DEXA uses ionising radiation and is therefore not appropriate for measurements during pregnancy.
Table 3 Characteristics of multi-component models.
| Consideration | Comment |
|---|---|
| Number of participants | Small |
| Relative cost | High |
| Participant burden | High as several techniques are required |
| Researcher burden of data collection | High as several techniques are required |
| Researcher burden of coding and data analysis | High |
| Risk of reactivity bias | No |
| Risk of recall bias | No |
| Risk of social desirability bias | No |
| Risk of observer bias | No |
| Space required | High |
| Availability | Medium |
| Suitability for field use | Low |
| Participant literacy required | No |
| Cognitively demanding | No |
Considerations relating to the use multi-component models in specific populations are described in Table 4.
Table 3 Use of multi-component models in different populations.
| Population | Comment |
|---|---|
| Pregnancy | 3C models are typically used as DEXA (required for 4C) is not feasible (ionizing radiation )*. |
| Infancy and lactation | Suitable. |
| Toddlers and young children | Suitable (3C approach might be used more often as the use of DEXA in this population can be challenging). |
| Adolescents | Suitable. |
| Adults | Suitable. |
| Older Adults | Suitable. |
| Ethnic groups | Suitable. |
| Other (obesity) | Suitable. |
*Forsum et al. (2014).
Refer to section: practical considerations for objective anthropometry
- Expertise in the various techniques used to derive body weight, volumes and densities.
- All the resources listed in the different methods used to derive multicomponent models are also applicable.
A method specific instrument library is being developed for this section. In the meantime, please refer to the overall instrument library page by clicking here to open in a new page.
- Delisle Nystrom C, Henriksson P, Alexandrou C, Lof M. The Tanita SC-240 to Assess Body Composition in Pre-School Children: An Evaluation against the Three Component Model. Nutrients. 2016;8(6). Epub 2016/06/21
- Elia M: Body composition analysis: an evaluation of 2 component models, multicomponent models and bedside techniques Clinical Nutrition 1992: 11; 114
- Ellis KJ: Human Body Composition: In Vivo Methods. Physiological Rev. 2000: 80; 649
- Fields DA, Goran MI: Body composition techniques and the four-compartment model in children Journal of Applied Physiology 2000: 89; 613
- Forsum E, Henriksson P, Lof M. The two-component model for calculating total body fat from body density: an evaluation in healthy women before, during and after pregnancy. Nutrients. 2014;6(12):5888-99. Epub 2014/12/20
- Fuller NJ,Jebb SA, Laskey MA: Four-component model for the assessment of body composition in humans: comparison with alternative methods, and evaluation of the density and hydration of fat-free mass. Clin Sci 1992: 82, 68
- Heymsfield SB, Ebbeling CB, Zheng J, Pietrobelli A et al: Multi-Component Molecular-Level Body Composition Reference Methods: Evolving Concepts and Future Directions Obesity Reviews 2015: 16; 282
- Heyward VH: Evaluation of body composition. Current issues. Sports Med 1996: 22; 146
- Lee SY, Gallagher D: Assessment methods in human body composition Current Opinion Clinical Nutr Metab Care 2008: 11; 566
- Lee SY, Gallagher D. Assessment methods in human body composition. Current opinion in clinical nutrition and metabolic care. 2008;11(5):566-72. Epub 2008/08/08
- Morgan MY, Madden AM, Jennings G, Elia M, Fuller NJ. Two-component models are of limited value for the assessment of body composition in patients with cirrhosis. The American journal of clinical nutrition. 2006;84(5):1151-62. Epub 2006/11/10
- Van Der Ploeg GE, Withers RT, Laforgia J. Percent body fat via DEXA: comparison with a four-compartment model. Journal of applied physiology. 2003;94(2):499-506. Epub 2003/01/18
- Wang ZM, Shen W, Withers RT, Heymsfield SB. Multicomponent molecular level model of body composition analysis. In: Heymsfield SB, Lohman TG, Going SB, editors.Human Body Composition. Human Kinetics; IL, Champaign: 2005. pp. 163–76
- Wells JC, Fewtrell MS. Measuring body composition. Archives of disease in childhood. 2006;91(7):612-7. Epub 2006/06/23
- Wells JC, Fuller NJ, Dewit O, Fewtrell MS, Elia M, Cole TJ. Four-component model of body composition in children: density and hydration of fat-free mass and comparison with simpler models. The American journal of clinical nutrition. 1999;69(5):904-12. Epub 1999/05/08
- Withers RT, LaForgia J, Pillans RK, Shipp NJ, Chatterton BE, Schultz CG, et al. Comparisons of two-, three-, and four-compartment models of body composition analysis in men and women. Journal of applied physiology. 1998;85(1):238-45. Epub 1998/07/09
A method specific instrument library is being developed for this section. In the meantime, please refer to the overall instrument library page by clicking here to open in a new page.

- The Toolkit
- About
- What's new
- Other resources
- Toolkit Team
- Contact
- Links to other toolkits
- Nutritools
- NCI/NIH Dietary Assessment Primer
- © 2026 MRC Epidemiology Unit
- Privacy policy and cookies
- Terms of Use